If you’re interested in contributing a short What Am I Reading post, we’d love to hear from you! Email us at cache@colorado.edu
Written by Sara Curran and June Yang, University of Washington
Research on disasters and health has increasingly leveraged linked administrative claims data and detailed spatial information on natural disaster events in order to move beyond single-case descriptions toward quasi-experimental designs. Such linkages aim to improve knowledge about the proximate mechanism (such as health care utilization) that link the consequence of disasters to health outcomes. Such insights about the mechanisms can then help target improvements for resilience and adaptation in the future. For example, a recent study of Puerto Rico integrated private insurance claims and beneficiary counts from multiple insurers to construct harmonized region–year indicators of infectious disease, injury, and mental health service use, and then interpreted abrupt shifts in these indicators around hurricanes, earthquakes, and the COVID-19 pandemic as signatures of disaster-related disruption to health care access and need (Stimpson et al., 2025). Building on the same logic of combining high-resolution utilization data with externally defined measures of hazard exposure and loss, another study links national Medicare fee-for-service claims with standardized disaster databases to estimate the short-term effects of extreme weather events on morbidity and mortality across U.S. counties (Salas et al., 2024). We summarize each article here and then offer a few suggestions for future research.
Stimpson et al. (2025) innovatively developed a harmonized repeated, cross-sectional insurance claims dataset from 2016-2022 in Puerto Rico. The aggregated data included information from each region and year about injuries, infectious diseases, mental health, and substance use claims and was standardized by the number of beneficiaries per region and year. The annual trend lines for each type of claims category are descriptively evaluated for each region. Following Hurricane Maria, they find in the affected regions larger or higher increases in claims related to infectious disease, injury, mental health, and substance use. Regions that were less impacted by Hurricane Maria showed lower rates of claims across all types. The authors argue that the data point to the need for targeted interventions to enhance overall infrastructure, especially health care infrastructure for improved health outcomes. The Stimson et al. study is a good example of creatively generating valuable evidence from insurance claims data to descriptively observe trends and patterns. The limitations of the study’s results are in the relatively small number of cases (region-year), making it impossible to statistically evaluate whether the differences are significant.
With a similar motivation for attention to study design, a recent article by Renee Salas and colleagues published in Nature Medicine creatively links NOAA and SHELDUS (Spatial Hazards and Economic Loss Data in the US) to Medicare fee-for-services administrative data to evaluate the impact of extreme weather events on health outcomes. The study examines counties impacted by at least one of 42 NOAA-identified, extremely damaging events (damages a total value of US$ 1 billion or higher), occurring between 2011 and 2016, and seeks to understand whether health outcomes changed in unaffected and affected counties before and after the event. They use the SHELDUS data to identify county-level damages for affected counties (the property and crop damages for those affected counties ranges between $3,220-$12.51 billion per county). Combined with the CMS data at the county-level they systematically compare affected and non-affected counties. This valuable quasi-experimental design offers a careful comparison across time evaluating impacts the week following a disaster, 1-2 weeks after, and 3-6 weeks after. These spatial and temporal comparisons across the entire country, offer an important national assessment of the immediate and lagged health outcome effects of severe weather events. Notably, the study limits itself to floods, severe storms, and winter storms, which, they argue, are events that are relatively short-lived, destroy infrastructure, and can have lingering social and built environment effects. They contrast these events to wildfire and droughts which often last for hundreds of days and have somewhat different impacts on infrastructure, so the authors do not evaluate these types of events and also exclude counties experiencing them from eligibility in the selection of matched control counties. They make two sets of comparisons. First, they compare the relative change in health outcomes in affected counties before and after events. Second, they compare similar counties with and without exposure to the event using a difference-in-difference estimation. They find similar results with both types of comparisons.
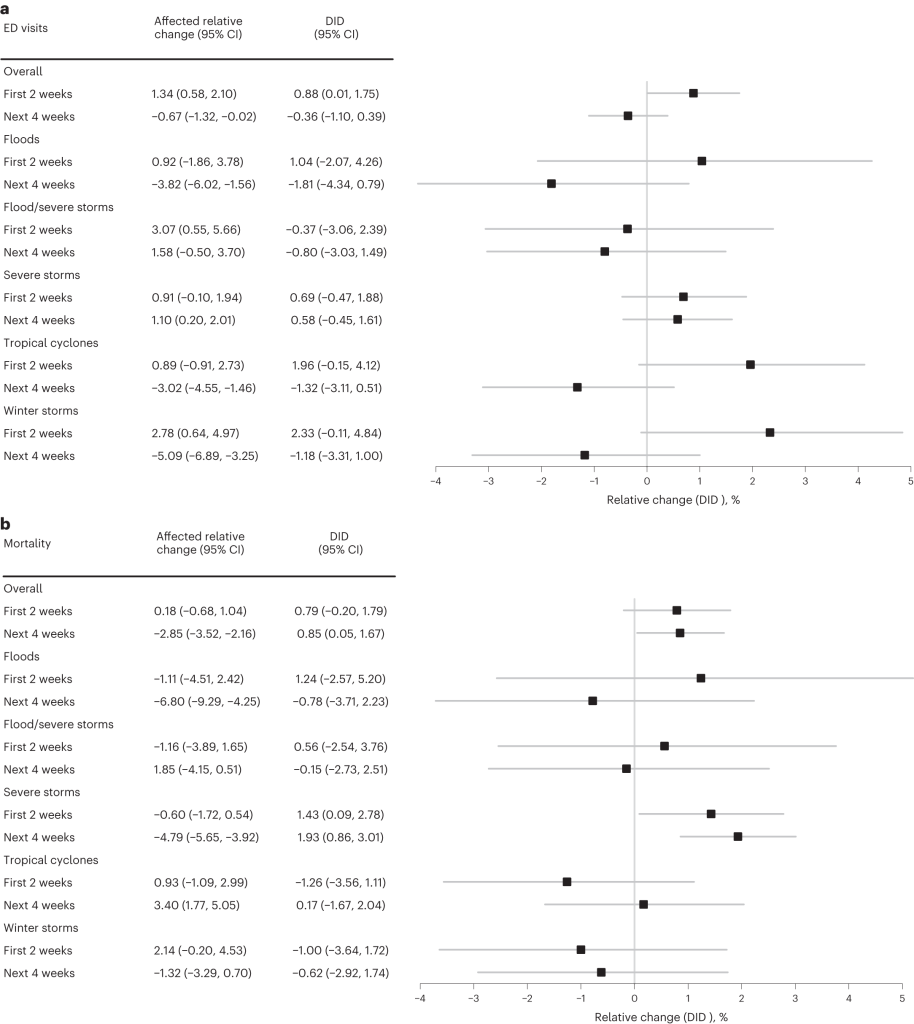
Fig. 2: Forest plots of ED visit and mortality relative change and DID for affected counties in post-disaster weeks 1–2 and weeks 3–6 in Medicare beneficiaries exposed to a short-term NOAA NCEI billion-dollar weather disaster in the United States. (Salas et al., 2024)
Winter storms and tropical cyclones are most damaging to health outcomes
Their most important findings are summarized in their Figure 2. They show how emergency department visits and mortality are significantly increased by severe events. In Panel a. emergency department visits are significantly higher in the first two weeks following a severe event, but not so in the weeks 4 or more. Most of these differences are driven by severe winter storms and tropical cyclones. In Panel b. mortality is significantly higher across all time lags. This mortality effect is primarily driven by severe storm events. Not shown in Figure 2, but discussed elsewhere, is the finding that non-elective hospitalizations remained unchanged over all types of severe storms and all the time lags. Besides demonstrating how particular types of severe events cause significant increases in emergency department visits and mortality, they also show that among storms totaling more than 1 US $ Billion in damages overall, the most expensive storm events are the ones driving the results (those in the upper quartile of counties (damages ranging between $622.66K-12.51B)).
This analyses and the linked data, together with Stimpson et al. (2025) study, suggest many useful avenues for further research that could leverage routinely collected administrative and claims data to understand the more precise and proximate mechanisms of health care utilization and costs of disasters on the US economy and health, and well-being of the US population. Future work can build on these designs to probe the mechanisms that generate vulnerability, such as pre-existing comorbidities, healthcare access barriers, and disruptions to utilities or transportation, and to identify which communities are more, or less resilient in the face of weather shocks.
Both studies reviewed here highlight the importance of understanding crucial heterogeneity of geography and preparedness impacting health care needs and capacities: for example, winter storms may be especially deadly in places like Texas where infrastructure and housing are optimized for heat rather than cold. Such geographic variation almost certainly intersects with social disadvantage, race, income, and other axes of inequality, suggesting that analyses that explicitly consider these overlapping vulnerabilities in relation to hazard exposure, built environment, and structural conditions are a critical next step. By expanding this line of inquiry to additional disaster types and contexts, researchers can generate evidence that not only clarifies patterns of risk, but also informs theory and policy on the social determinants of disaster vulnerability, resilience, and health system performance.
For those interested, code for Salas et al. (2024) is available at GitHub and can be found at https://github.com/Billion-Dollar-Weather-Medicare/ED-Hospitalizations-Mortality/.
Notes about administrative data:
“Administrative data” here means records generated during the routine administration of healthcare and insurance, for example, billing/claims files, enrollment and beneficiary summary files, and facility or provider administrative records. These datasets are not collected for research, but capture large populations and longitudinal events (visits, diagnoses, procedures, dates and place of care), which makes them powerful for measuring changes in utilization, costs, and short-term outcomes after disasters, while also carrying limitations (limited clinical detail, timing/coverage constraints, and privacy/regulatory restrictions).
Salas et al. (2024) used fee-for-service Medicare administrative claims and beneficiary files to measure ED visits, hospitalizations, and mortality after billion-dollar weather disasters (these Medicare files are controlled by Center for Medicare & Medicaid Services and cannot be redistributed by the authors). Stimpson et al. (2025) analyzed private insurance claims for Puerto Rico obtained through the territory’s Office of the Commissioner of Insurance, illustrating how regulator-level aggregates from insurers can be used to study regional patterns after consecutive disasters.
References
-
Salas, Renee, Laura Burke, Jessica Phelan, Gregory Wellenius, E. John Orav, & Ashish Jha. 2024. “Impact of Extreme Weather Events on Healthcare Utilization and Mortality in the U.S.” Nature Medicine https://doi.org/10.1038/s41591-024-02833-x
-
Stimpson, Jim P., Damaris Lopez Mercado, Alexandra C. Rivera-González, Jonathan Purtle, and Alexander N. Ortega. 2025. “A Regional Analysis of Healthcare Utilization Trends during Consecutive Disasters in Puerto Rico Using Private Claims Data.” Scientific Reports 15(1):5249. doi:10.1038/s41598-025-89983-1.