If you’re interested in contributing a short What Am I Reading post, we’d love to hear from you! Email us at cache@colorado.edu.
Written by Eun Young Choi, Postdoctoral Associate, University of Southern California
High temperatures are heating not only our neighborhoods and homes, but also our very biology, as we suggested in a recent study (Choi & Ailshire, 2025). Among the many ways extreme heat threatens public health, its subtle yet significant impact on the body’s aging processes has begun to draw attention. I’ve been exploring how we can quantify the biological consequences of extreme heat, and why these hidden impacts matter for aging research.
Why Focus on Biological Aging?
Much of the climate-health literature has understandably focused on observable health outcomes: hospitalizations, respiratory and cardiovascular diseases, and death (Bunker et al., 2016; Hajat et al., 2010). These are essential indicators, but the effects of extreme heat might not immediately manifest as diagnosable conditions; instead, they may exert a silent toll at the cellular and molecular level. Over time, this biological strain can accumulate, increasing the risk of disability and disease. Biological age, measured using biomarkers that reflect physiological wear and tear, offers a promising way to identify early signs of changes in the body before chronic conditions are formally diagnosed. These include measures based on clinical biomarkers, cellular markers, and, more recently, molecular signatures such as DNA methylation (Chen et al., 2023 for review). Each of these tools provides a useful lens into how the aging process may advance more rapidly than expected based on chronological age, and how it may be shaped by external stressors like heat. Recent studies show that accelerated biological aging is associated with elevated risk of cardiovascular disease, cognitive decline, and mortality (Emami et al., 2022; Fransquet et al., 2019; Zhou et al., 2022). As such, these clocks provide a useful intermediate endpoint that can be particularly valuable when studying environmental exposures, which often unfold gradually and exert diffuse effects across multiple body systems. In this context, biological age can help us understand not just whether heat is harmful, but how it does its damage.
How Do We Measure Heat?
Measuring exposure to extreme heat may appear straightforward, but it involves multiple layers of complexity. The most common metric is ambient temperature (technically, the temperature in the surrounding environment), but even this can be defined in various ways—daily maximums, minimums, or averages—and it usually refers to outdoor air temperature. Others use composite indices that better approximate heat stress on the human body. The Heat Index, for example, incorporates humidity and is used to estimate heat-related stress in shaded environments (National Weather Service). The Wet-Bulb Globe Temperature (WBGT) goes further by accounting for wind speed, cloud cover, and sun angle as well to reflect conditions in direct sunlight, making it especially relevant for outdoor or occupational settings. Each of these measures captures different aspects of thermal stress, and the choice of metric should align with the study’s research question and target population. In our study, we used the Heat Index because our sample consisted of older adults, who are generally less likely to work outdoors or spend extended time in full sun. While these metrics can technically be measured indoors, they are typically based on outdoor weather data and do not directly reflect indoor conditions.
How Can We Conceptualize Outdoor Heat Exposure to Better Estimate Health Impacts?
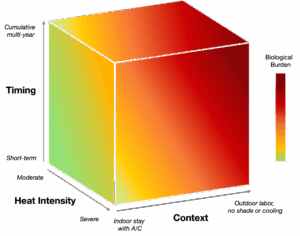
Researchers have considered a variety of factors to understand the magnitude of heat-related health effects. Here, I created a conceptual cube with three axes to synthesize commonly used dimensions: exposure timing, heat intensity, and exposure context. This framework is not a modeling tool, but rather a way to clarify how different features of outdoor heat exposure interact to shape physiological burden.
- Y-axis: What timeframe is captured?
Exposure can occur over various timeframes: a single hot day, a multi-day heatwave, or repeated seasonal exposures over years. Short-term heat events can trigger immediate physiological stress responses (e.g., inflammation), while longer-term exposure to elevated temperatures may produce cumulative biological wear and tear. Studies use various time windows to model these effects, from several day lags to multi-year averages, depending on the health outcome of interest. While short-term physiological responses to heat stress may be transient, some effects may accumulate over time and this continuous exposure may leave biological imprints detectable by biomarker-based measures. For example, our findings show consistent associations between longer-term heat exposure (e.g., 1-year and 6-year cumulative heat days) and accelerated epigenetic aging, consistent with prior studies reporting robust associations and large effect sizes for longer-term heat exposure (Chiu et al., 2024; Ni et al., 2023).
- Z-axis. How severe is the exposure?
This axis represents the intensity of the heat experienced. Researchers use both relative and absolute metrics to define extreme heat. Relative measures, such as temperatures above the 95th percentile of the local historical distribution, are useful for identifying deviations from the norm, especially considering that long-term sublethal heat can lead to physiological adaptations and increased thermal tolerance (Carr et al., 2024; Périard et al., 2016). In contrast, absolute thresholds (e.g., >95°F or >35°C) provide a fixed reference point that can be useful for identifying biologically hazardous temperatures and facilitating comparisons across regions. For the Heat Index, for example, the National Weather Service offers a practical classification: 80°F (Caution), 90°F (Extreme Caution), and 103°F (Danger). The choice between relative and absolute measures should be guided by the study’s objective, the population’s vulnerability, and the geographic and climatic context.
- X-axis. How is exposure experienced?
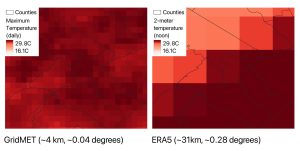
This axis reflects the context: the individual or situational factors that influence how ambient heat translates into actual personal exposure. Most studies use outdoor temperature data from weather stations or modeled products, and these measures may not fully capture personal exposure – a challenge also seen in air pollution research, where ambient data often serve as proxies for individual exposure (see related discussion). It is therefore important to interpret such data as approximating the potential for exposure rather than direct experience. Key contextual modifiers include time spent outdoors, occupational exposure, housing quality, and access to cooling resources. For instance, older adults living in poorly insulated homes without air conditioning may experience disproportionately high indoor heat, despite similar ambient temperatures. Recent work has also highlighted substantial within-neighborhood variation in heat exposure, reinforcing the need to consider behavioral and environmental mediators when interpreting ambient heat metrics (Li et al., 2023; Reid et al., 2009).
The color gradient in the figure reflects increasing physiological burden, illustrating how these dimensions can intersect to magnify biological stress. For instance, someone who works outdoors (high context), over many years (longer timing), and in areas where temperatures regularly exceed 100°F (high intensity), may experience substantially greater heat-related aging than someone briefly exposed to moderate heat while indoors.
What We Found about Heat and Epigenetic Aging
There is growing evidence from animal studies that heat stress can trigger epigenetic alterations such as DNA methylation, positioning these molecular changes as a plausible biological mechanism linking environmental exposures to long-term health outcomes (Murray et al., 2022). Epigenetic clocks—biological age estimates derived from DNA methylation levels across the genome—can capture cumulative physiological responses to stress and toxins. In our work, we’ve begun to apply these epigenetic measures to understand how outdoor heat exposure may accelerate epigenetic aging. Our findings show that outdoor heat, especially long-term, was significantly associated with greater acceleration in epigenetic age in a diverse national cohort of older adults. These associations persisted even after adjusting for individual-level socioeconomic and behavioral factors, as well as community-level characteristics. Taken together, these findings suggest that chronic heat exposure may not only increase immediate health risks but also disrupt key systems contributing to a steeper trajectory of epigenetic aging, potentially through pathways involving oxidative stress, inflammation, and metabolic reprogramming (Murray et al., 2022). Nonetheless, further evidence is needed to clarify the specific mechanisms linking heat exposure to epigenetic aging acceleration.
Moving Forward
Advancing this research requires embracing the complexity of both exposures and outcomes. On the exposure side, we must better account for co-occurring environmental stressors. Heat rarely acts alone. For instance, air pollution tends to worsen on hot days, creating compound exposures that may have synergistic effects on biological systems. We also need more attention to contextual variation, how housing, neighborhood infrastructure, and access to cooling resources shape actual heat burden experienced by older adults. This is especially pressing in low-income or racially marginalized communities, where systemic disinvestment may amplify risk. On the outcome side, biological aging is multidimensional. While epigenetic clocks help pinpoint biological responses to heat across systems, they capture only part of the picture. It remains unclear how—and to what extent—heat stress affects specific systems such as the immune, neuro, metabolic, cardiovascular, and renal systems in large human samples. Integrating additional biomarkers such as inflammatory cytokines, neurodegenerative markers, and metabolomic signatures can help build a more comprehensive understanding of how heat “ages” us biologically.
Final Reflections
Extreme heat is no longer exceptional—it is a defining feature of our climate reality. To understand its full toll on aging populations, we must look beyond acute events and capture the long-term, cumulative effects of chronic stress. Biological aging measures offer an important window into these processes, enabling earlier detection, monitoring of intervention impacts, and deeper insight into vulnerability. But how we measure exposure and aging matters. Choices about metrics and methods shape our conclusions—and our ability to act. Integrating high-resolution environmental data with multidimensional biomarkers will be key to building a fuller picture of how climate shapes the aging process.
References
Choi EY, Ailshire JA. Ambient outdoor heat and accelerated epigenetic aging among older adults in the US. Sci Adv. 2025;11(9):eadr0616. doi:10.1126/sciadv.adr0616
Bunker A, Wildenhain J, Vandenbergh A, et al. Effects of Air Temperature on Climate-Sensitive Mortality and Morbidity Outcomes in the Elderly; a Systematic Review and Meta-analysis of Epidemiological Evidence. eBioMedicine. 2016;6:258-268. doi:10.1016/j.ebiom.2016.02.034
Hajat S, O’Connor M, Kosatsky T. Health effects of hot weather: from awareness of risk factors to effective health protection. The Lancet. 2010;375(9717):856-863. doi:10.1016/S0140-6736(09)61711-6
Chen R, Wang Y, Zhang S, et al. Biomarkers of ageing: Current state-of-art, challenges, and opportunities. MedComm – Future Medicine. 2023;2(2):e50. doi:10.1002/mef2.50
Emami M, Agbaedeng TA, Thomas G, et al. Accelerated Biological Aging Secondary to Cardiometabolic Risk Factors Is a Predictor of Cardiovascular Mortality: A Systematic Review and Meta-analysis. Canadian Journal of Cardiology. 2022;38(3):365-375. doi:10.1016/j.cjca.2021.10.012
Fransquet PD, Wrigglesworth J, Woods RL, Ernst ME, Ryan J. The epigenetic clock as a predictor of disease and mortality risk: a systematic review and meta-analysis. Clin Epigenet. 2019;11(1):1-17. doi:10.1186/s13148-019-0656-7
Zhou A, Wu Z, Zaw Phyo AZ, Torres D, Vishwanath S, Ryan J. Epigenetic aging as a biomarker of dementia and related outcomes: a systematic review. Epigenomics. 2022;14(18):1125-1138. doi:10.2217/epi-2022-0209
National Weather Service, Wet Bulb Globe Temperature vs Heat Index. https://www.weather.gov/ict/WBGT.
Chiu KC, Hsieh MS, Huang YT, Liu CY. Exposure to ambient temperature and heat index in relation to DNA methylation age: A population-based study in Taiwan. Environment International. 2024;186:108581. doi:10.1016/j.envint.2024.108581
Ni W, Nikolaou N, Ward-Caviness CK, et al. Associations between medium- and long-term exposure to air temperature and epigenetic age acceleration. Environment International. 2023;178:108109. doi:10.1016/j.envint.2023.108109
Deborah Carr, Giacomo Falchetta, Ian Sue Wing, Population Aging and Heat Exposure in the 21st Century: Which U.S. Regions Are at Greatest Risk and Why?, The Gerontologist, Volume 64, Issue 3, March 2024, gnad050, https://doi.org/10.1093/geront/gnad050
Périard JD, Travers GJS, Racinais S, Sawka MN. Cardiovascular adaptations supporting human exercise-heat acclimation. Autonomic Neuroscience. 2016;196:52-62. doi:10.1016/j.autneu.2016.02.002
Li A, Toll M, Bentley R. Mapping social vulnerability indicators to understand the health impacts of climate change: a scoping review. The Lancet Planetary Health. 2023;7(11):e925-e937. doi:10.1016/s2542-5196(23)00216-4
Reid CE, O’Neill MS, Gronlund CJ, et al. Mapping Community Determinants of Heat Vulnerability. Environ Health Perspect. 2009;117(11):1730-1736. doi:10.1289/ehp.0900683
Murray KO, Clanton TL, Horowitz M. Epigenetic responses to heat: From adaptation to maladaptation. Experimental Physiology. 2022;107(10):1144-1158. doi:10.1113/EP090143